
Proteinuria in Pregnancy
During pregnancy, proteinuria has traditionally been a hallmark of preeclampsia, but it is also a nonspecific indicator of renal disease and may result from an elevated plasma protein concentration, increased glomerular permeability, decreased tubular protein reabsorption, and renal hemodynamic alterations. It has been reported that the rate of isolated proteinuria in pregnancy may reach 8%, whereas preeclampsia occurs among 3% to 8% of pregnancies.
When a pregnant woman urinary protein excretion surpasses 300 mg/24 hours at any point during her pregnancy, it is deemed abnormal; this quantity often corresponds to a 1+ on a urine dipstick. Before 20 weeks of gestation or before becoming pregnant, proteinuria may indicate the presence of renal illness.
Causes of Proteinuria in Pregnancy
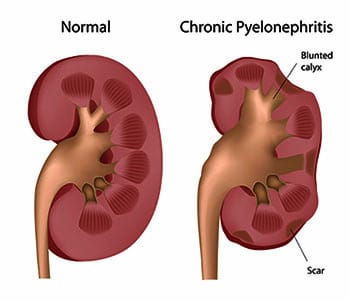
- Kidney Infections
- Primary Kidney Disease
- Diabetes
- Several Pregnancies
- Chronic Hypertension (persistent high blood pressure)
- Immune system diseases
Diagnosis of Proteinuria in Pregnancy
- 24-hours Urine Collection
- Dipsticks for Urine
- Monitoring of Blood Pressure
- Typical Urinalysis
- Ultrasound to assess renal function and look for any anomalies that could be the source of proteinuria.
- Blood Tests
Treatment of Proteinuria in Pregnancy
- Bed Rest when a patient had preeclampsia, doctors used to frequently recommend bed rest. Regarding this is effectiveness, however, opinions differ. A higher risk of blood clots, together with other social and economic concerns, have led to the general recommendation against bed rest.
- Frequent Monitoring in order to track any changes in your health or the health of your unborn child, your doctor probably wants you to come in for testing more frequently.
- Nutritional Changes A healthy, well-balanced diet that includes enough protein is essential. Specific dietary advice, however, must to be explored with a medical professional.
- Blood Pressure Control when blood pressure is extremely high, antihypertensives can be used to decrease it. There are choices that are secure to use when expecting.
If preeclampsia is severe, delivery can be the only course of action. Your doctor may administer one or two corticosteroid injections, spaced 24 hours apart, to assist grow your unborn child’s lungs in the event that an early birth is necessary.
If you don’t get preeclampsia treated, you may be at increased risk for problems such as placental abruption, heavy bleeding, stroke, or seizures. Preeclampsia can be fatal in certain situations. For this reason, it is very important to work closely with your healthcare practitioner if you develop any symptoms.